Why Are MHA Detention Rates So Different Across England? A Closer Look for AMHPs
By Matilda Minchin
Results of a Study looking at Large Variation in Rates of Mental Health Act (MHA) Detention Across England
In this blog, I will discuss the above study which I conducted with a team at UCL, looking at variation in the rates of Mental Health Act (MHA) detention across England. Using data from 2021/22, we found a four-fold difference between the areas in England with the highest and lowest rates of MHA detention. Only 11% of this variance was explained by the demographic and clinical variables we used in our study, the rest being unexplained. I wanted to share these findings with AMHPs as the professionals making these decisions, so we can think about why we are seeing this variation. I’ll first share some research that has looked at variation in use of the MHA across England. I’ll then talk about our study and what we found in more detail.
Using data on MHA use in England from 2010/11, two studies found that areas with higher deprivation, higher urbanicity, and higher ethnic diversity had higher rates of involuntary detention (2,3). This makes sense with what we know about who may be more likely to experience mental illness or be detained under the MHA (4). When looking at ethnicity specifically, there is an overrepresentation of people from ethnic minority groups in MHA detentions in the UK, specifically Black Caribbean and Black African people (5). Some reasons for this could include healthcare inequalities when accessing appropriate community care, bias in perceived risk of violence, and higher police contact. However, these studies found that most of the variation in MHA detentions across England was unexplained by the demographic factors they included in their research. Some key factors that they did not use, including the level of mental illness in the population of each area, may explain some of this variation.
To explore this further, we set out to reassess variation in MHA use across England, using data from the 2021/22 MHA detention statistics of the Mental Health Services Data Set (6). Using more recent data than other studies allowed us to account for changes in demographics and government policies that have substantially influenced mental health care provision in England in the past 10 years. We looked at variation across Clinical Commissioning Groups (CCGs: the NHS bodies responsible for planning and delivering healthcare across England before being replaced by Integrated Care Boards in 2022). We used factors previously seen to be linked to involuntary detention rates: severe mental illness, young age (18 to 35 years), male sex, non-White ethnicity, deprivation, urbanicity, and community and outpatient service use. The levels of each of these variables in each CCG was compared to the rate of MHA detentions in each area. We used data on the population of these areas, for example the % of people living in urban areas in a CCG, not data from individuals. This means that this study cannot be used to assess the impact of different risk factors on the chances of an individual being detained.
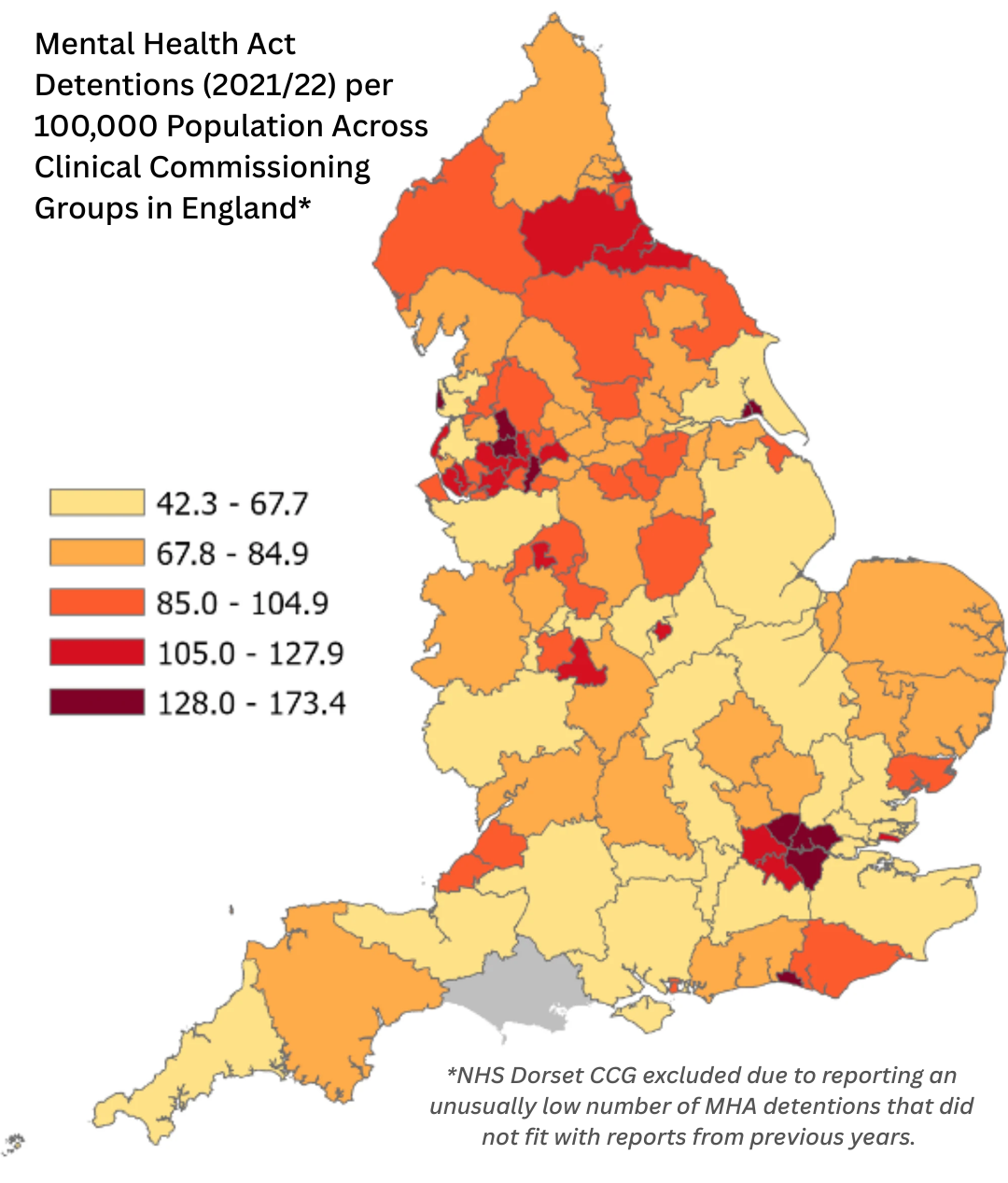
The rate of MHA detentions ranged from 42.30 per 100,000 population in NHS Surrey Heartlands CCG to 173.40 in NHS Blackpool CCG, with an average of 88.97 per 100,000. The below map shows the rate of MHA detentions across CCGs in England.
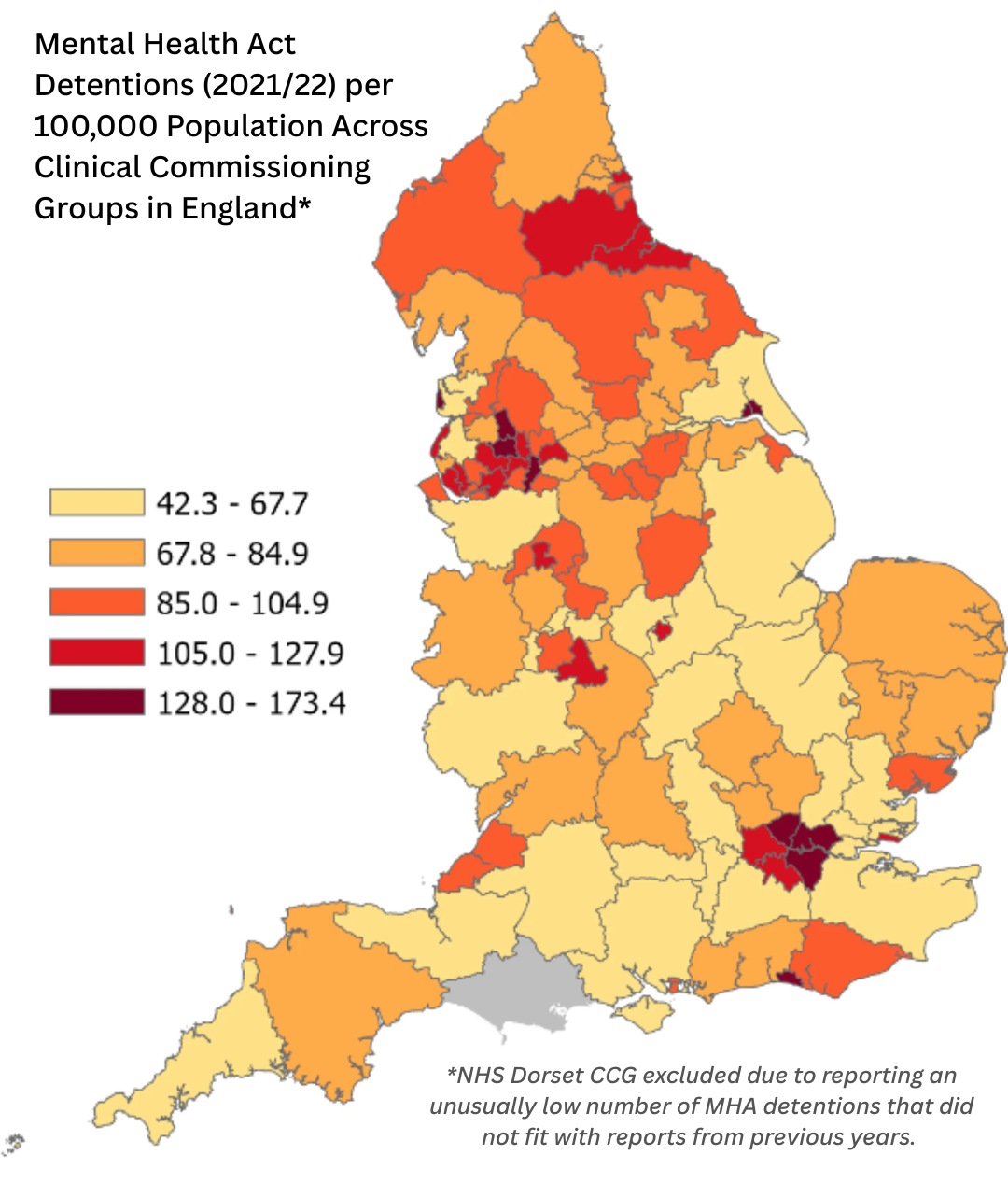
Map created using 2021/22 MHA detention statistics of the Mental Health Services Data Set (6) and CCG boundaries (April 2021) from Open Geography Portal (https://geoportal.statistics.gov.uk/).
The variables in our study only explained 11% of the variation in MHA detentions between CCGs, with the remaining variance being unexplained. This variance was large, with a four-fold difference between the CCGs with the highest and lowest rate of MHA detentions. Differences in service provision and implementation of the MHA, which we couldn’t measure, may explain some of the remaining difference between areas. It is important to examine these differences in future research, as it may highlight overuse or misuse of the MHA.
In terms of individual factors, the level of severe mental illness in an area was strongly related to the rate of MHA detentions when controlling for all other factors. For each standard deviation* increase in the percentage of severe mental illness in the population (0.17%), the rate of MHA detentions increased by 22.56%. On top of this, the number of community and outpatient mental health visits in an area was strongly related to the rate of MHA detentions. For each standard deviation increase in the number of community and outpatient mental health visits (8.25 per 100 population), the rate of MHA detentions increased by 10.73%. This means that more community contacts were associated with more MHA detentions after controlling for all other variables, including the level of severe mental illness in the population. This is a concerning finding as greater access to community treatment should reduce the need for involuntary inpatient care. Some previous research has similarly found that higher community healthcare spending and better community services are linked to higher involuntary detention (3,7). It could be the case that greater access to community treatment means those in need of involuntary detention are better identified, but more research needs to be done to fully understand this.
Finally, the percentage of male population in an area was moderately associated to the rate of MHA detentions. For each standard deviation increase in the percentage of males in the population (0.63%), the rate of MHA detentions increased by 5.36%. Male gender is consistently linked to increased MHA detention and could reflect higher perceived dangerousness or lack of help-seeking behaviour (8).
We did not find higher urbanicity, deprivation, percentage of population aged 18 to 35, or percentage of population of non-White ethnicity to be associated with higher involuntary detention. This differs from the findings of previous work. It could suggest that these factors do not affect involuntary detention when other variables, including severe mental illness, are taken into account. However, complex relationships between these variables and mental illness may complicate our results. When we try to understand the individual contribution of each variable on MHA detentions, all other variables in the model are kept at the same level. As these variables have complex relationships, this process may have flattened each variable’s association with MHA detentions. Future research should aim to disentangle these relationships, ideally using methods that look at data over time, to better understand how these variables interact with MHA detention.
Summary: The rate of MHA detentions varies greatly between geographical areas of the UK. Characteristics of an area that were associated with higher MHA detentions in this study include higher proportion of the population with severe mental illness, higher rates of community contacts, and higher male population. The population characteristics we were able to include in the analysis only accounted for 11% of the variation in MHA detentions. It is important to think about what might be causing the rest of this variation.
*Standard deviation measures the spread that observations show from the mean value of a variable. In a normally distributed variable (where an even number of observations fall above and below the mean), 68% of observations would fall one standard deviation above or below the mean, and 95% would fall within two standard deviations above or below the mean. Therefore a “standard deviation increase” means a jump from 0 to 1 standard deviations from the mean, or a jump from 1 to 2 and so on.
References used in this blog
1. Sheridan Rains L, Zenina T, Dias MC, Jones R, Jeffreys S, Branthonne-Foster S, et al. Variations in patterns of involuntary hospitalisation and in legal frameworks: an international comparative study. The Lancet Psychiatry. 2019;6(5).
2. Keown P, McBride O, Twigg L, Crepaz-Keay D, Cyhlarova E, Parsons H, et al. Rates of voluntary and compulsory psychiatric in-patient treatment in England: An ecological study investigating associations with deprivation and demographics. Br J Psychiatry. 2016;209(2).
3. Weich S, McBride O, Twigg L, Duncan C, Keown P, Crepaz-Keay D, et al. Variation in compulsory psychiatric inpatient admission in England: a cross-classified, multilevel analysis. The Lancet Psychiatry. 2017;4(8).
4. Laporte D, Chilman N, Morgan C, Schofield P, Wykes T, Das-Munshi J. The association between area-level factors and mortality in severe mental illnesses: A systematic review. Vol. 264, Schizophrenia Research. 2024.
5. Barnett P, Mackay E, Matthews H, Gate R, Greenwood H, Ariyo K, et al. Ethnic variations in compulsory detention under the Mental Health Act: a systematic review and meta-analysis of international data. The Lancet Psychiatry. 2019 Apr;6(4):305–17.
6. NHS Digital. https://digital.nhs.uk/data-and-information/publications/statistical/mental-health-act-statistics-annual-figures. 2022. Mental Health Act Statistics, Annual Figures. NHS Digital.
7. Sheridan Rains L, Weich S, Maddock C, Smith S, Keown P, Crepaz-Keay D, et al. Understanding increasing rates of psychiatric hospital detentions in England: development and preliminary testing of an explanatory model. BJPsych Open. 2020;6(5).
8. Curley A, Agada E, Emechebe A, Anamdi C, Ng XT, Duffy R, et al. Exploring and explaining involuntary care: The relationship between psychiatric admission status, gender and other demographic and clinical variables. Int J Law Psychiatry. 2016;47.
Picture provided by owner Matilda Minchin